
Coviello et al.
Demonstrated that intratesticular testosterone can fall dramatically on testosterone alone, and that low-dose hCG can help preserve this local testicular hormone environment.
hCG on TRT is most commonly discussed in relation to fertility, intratesticular testosterone, and preservation of testicular function during testosterone replacement therapy. Human chorionic gonadotropin, usually shortened to hCG, can mimic luteinising hormone (LH), which is the pituitary signal that normally stimulates the testes to produce testosterone.
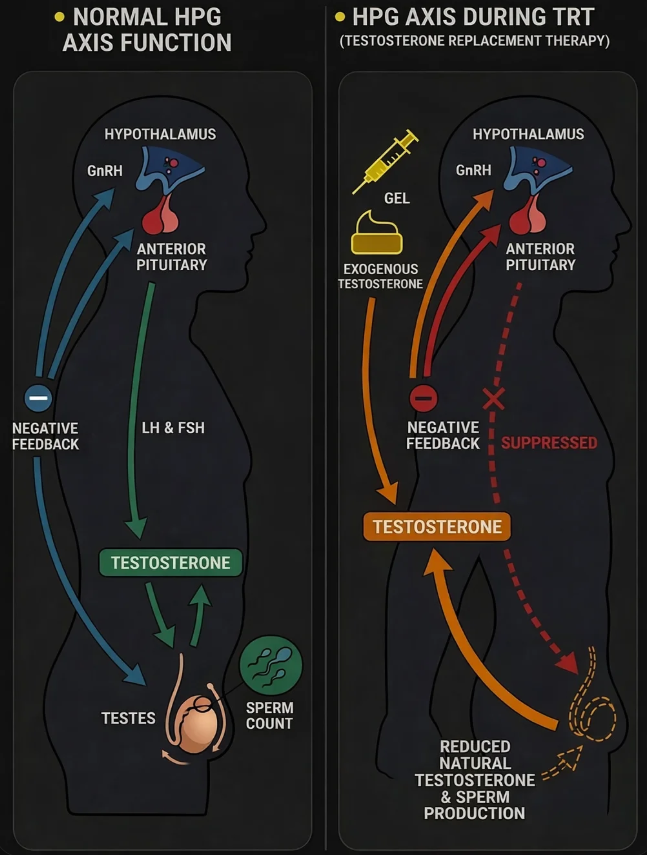
When men begin testosterone replacement therapy, testosterone is being supplied externally rather than produced entirely through the body’s usual signalling pathway. That change affects the hypothalamic-pituitary-gonadal (HPG) axis and often reduces LH and follicle-stimulating hormone (FSH) output from the brain.
Because LH stimulation falls, the testes receive less instruction to maintain internal testosterone production. Over time, that can reduce intratesticular testosterone, affect sperm production, and contribute to lower testicular activity. This is why hCG on TRT is often discussed in protocols where fertility or preservation of testicular function remains important.
This guide explains what hCG is, how hCG on TRT works, what happens to the HPG axis during testosterone therapy, and what current evidence suggests about fertility, hormones, and monitoring in the UK.
This page is educational only. It is not personal medical advice, and treatment decisions should always be made with appropriate clinical oversight.
hCG stands for human chorionic gonadotropin. It is best known for its role in pregnancy, but in male hormone medicine it is relevant because it can activate the same receptor pathway normally used by luteinising hormone.
LH is produced by the pituitary gland and stimulates Leydig cells within the testes to produce testosterone. Because hCG can act at the same receptor, it can mimic part of that signalling pathway when pituitary LH output has been reduced.
This is why hCG on TRT is discussed in fertility-preserving testosterone protocols. Testosterone therapy can improve circulating androgen levels, but it does not directly replace every part of the body’s normal reproductive signalling system.
If you want the broader treatment overview first, see the TRT UK guide.
Testosterone production is regulated through the hypothalamic-pituitary-gonadal axis. The hypothalamus releases gonadotropin-releasing hormone (GnRH), which stimulates the pituitary gland to release LH and FSH.
LH mainly stimulates Leydig cells to produce testosterone inside the testes. FSH is more closely linked to Sertoli cell function and the wider process of sperm development. These pathways are connected rather than separate, which means testosterone production and spermatogenesis depend on coordinated signalling.
This axis is controlled through feedback. When testosterone and oestradiol levels rise, the brain reduces GnRH, LH and FSH output. When they fall, signalling increases again. Understanding that feedback loop is essential when looking at how hCG on TRT works.
When testosterone is supplied externally through TRT, the body detects that androgen levels are already being maintained. In response, the hypothalamus and pituitary typically reduce their release of GnRH, LH and FSH.
This matters because the testes no longer receive the same level of stimulation they would under normal physiology. Even if blood testosterone levels look adequate on treatment, intratesticular testosterone can still fall sharply.
That suppression can affect sperm production and testicular activity over time. It is one of the main reasons hCG on TRT is discussed at all: hCG is used to replace part of the missing LH signal that testosterone alone does not provide.
For a broader introduction to treatment pathways, monitoring and diagnosis, read the main TRT UK guide.
Rather than supplying testosterone directly, hCG on TRT works by stimulating the testes through the luteinising hormone receptor. This helps preserve some internal testosterone production inside the testis while circulating testosterone is supported by therapy.
This distinction matters because serum testosterone and intratesticular testosterone are not the same. A man may have adequate testosterone levels in the bloodstream on TRT, but the local hormonal environment inside the testes can still be heavily suppressed if LH signalling has fallen away.
For that reason, hCG on TRT is mainly discussed in relation to preserving testicular activity, supporting fertility-related physiology, and maintaining part of the signalling pathway that external testosterone does not replace.
LH is naturally released in pulses and has a very short biological half-life. That makes it impractical as a routine replacement option in standard clinical settings.
hCG has a longer half-life and provides more sustained receptor stimulation. It is not chemically identical to LH, but it is sufficiently similar in receptor activity to be clinically useful when discussing hCG on TRT and preservation of testicular signalling.
One of the main reasons hCG on TRT is studied and discussed is fertility preservation. Sperm production depends on more than testosterone in the bloodstream. It also depends on sufficiently maintained intratesticular testosterone and coordinated testicular signalling.
During testosterone-only therapy, suppression of LH and FSH may reduce spermatogenesis over time. By stimulating Leydig cells, hCG can help support intratesticular testosterone levels that are relevant to sperm production.
This does not guarantee preserved fertility, and responses vary between individuals. However, research has shown that low-dose hCG used alongside TRT may help preserve semen parameters in some men where fertility remains an active treatment consideration.
If fertility planning is relevant, baseline testing and monitoring matter. For UK laboratory routes, Origin Bloods is one useful reference point.
Reduced testicular stimulation during testosterone-only therapy can affect more than fertility. It can also influence testicular volume and overall function. Many men notice some degree of testicular shrinkage when gonadotropin signalling is suppressed over time.
hCG is used in some protocols because it keeps the testes more active than testosterone monotherapy alone. That may help preserve testicular size and reduce the degree of functional shutdown associated with absent LH stimulation.
This is one reason hCG on TRT is discussed beyond fertility alone. For some men, maintenance of testicular activity remains relevant from both a physiological and quality-of-life perspective.
Although fertility preservation is the clearest and best-established reason for using hCG during testosterone therapy, it is not the only reason it is discussed. Some clinicians and patients also consider hCG as a way of maintaining a more complete physiological picture during treatment.
That usually means preserving some testicular steroidogenesis rather than relying entirely on external testosterone. Interest has also extended into libido, wellbeing and broader neuroendocrine function, although the evidence base here is less consistent than it is for fertility-related outcomes.
For that reason, the strongest factual case for hCG on TRT remains its role in supporting intratesticular testosterone and helping preserve aspects of reproductive function where clinically relevant.
Research on hCG on TRT generally focuses on preservation of intratesticular testosterone, maintenance of spermatogenesis, and broader support of testicular function during hormonal suppression.
Earlier work showed that exogenous testosterone alone can cause a major reduction in intratesticular testosterone. Later studies found that adding low-dose hCG could substantially blunt that decline, which helps explain why it has become an important point of discussion in fertility-preserving TRT protocols.
Clinical studies have also reported preserved semen parameters in some men using testosterone therapy alongside low-dose hCG. Study designs and protocols differ, but the overall direction of evidence supports hCG where fertility preservation is a meaningful treatment priority.
This is also consistent with discussion seen across recognised men’s health and sexual medicine frameworks, where fertility preservation is treated separately from testosterone replacement alone.
Demonstrated that intratesticular testosterone can fall dramatically on testosterone alone, and that low-dose hCG can help preserve this local testicular hormone environment.
Reported preserved semen parameters in men receiving testosterone therapy with low-dose hCG, supporting its relevance where fertility remains clinically important.
More recent publications continue to explore hCG-based approaches for restoring or supporting spermatogenesis in men affected by androgen-related suppression.
hCG is a prescription treatment and should only be used with appropriate medical supervision. As with any hormone-related therapy, the decision to include hCG on TRT depends on diagnosis, treatment goals, fertility plans, baseline bloodwork and an appropriate monitoring strategy.
Not every man on TRT needs hCG. Its relevance becomes greater where preserving fertility or maintaining some degree of testicular activity is part of the treatment objective.
Monitoring still matters. Testosterone, oestradiol, full blood count, PSA where appropriate, and wider metabolic or endocrine markers should be reviewed as part of a sensible protocol. You can read more in How TRT Monitoring Works.
For men exploring private UK treatment pathways, Origin TRT is one example of a clinic route where diagnosis, treatment and monitoring form part of a wider ongoing process.
hCG is not simply an add-on to TRT at random. Its main role is usually discussed in relation to fertility, intratesticular testosterone, and preservation of testicular function during treatment.
Even where hCG is used, treatment should not be reduced to a simple question of adding or removing one medication. Hormone care still depends on diagnosis, baseline testing, symptom review and structured follow-up.
That is especially important in the UK TRT setting, where patients often arrive with overlapping issues involving testosterone, SHBG, oestradiol, thyroid function, prolactin, metabolic health, and fertility concerns. If you want the broader testing picture, see Understanding TRT Bloodwork in the UK.
This page works best as part of a wider TRT UK knowledge hub around diagnosis, bloodwork, monitoring, symptoms and treatment pathways.
hCG is best understood as a tool used to preserve part of normal testicular signalling during testosterone therapy. Its strongest rationale is not that it simply “boosts” TRT, but that it can help preserve intratesticular testosterone and support fertility-related physiology when gonadotropin signalling has been suppressed.
For men researching TRT UK, UK TRT, and fertility-aware testosterone treatment, understanding hCG on TRT is an important part of understanding how hormone therapy affects the reproductive axis over time.
hCG on TRT mimics luteinising hormone and stimulates the testes, which can help preserve intratesticular testosterone during testosterone therapy.
Yes. Testosterone therapy commonly suppresses LH and FSH, which may reduce sperm production and lower intratesticular testosterone over time.
No. It is not essential in every protocol. Its role becomes more relevant when preserving fertility or maintaining testicular function is a treatment goal.
It is discussed because men researching TRT often want to understand not only testosterone levels, but also fertility, testicular function and the effects of long-term hormonal suppression.
You can explore broader testing through Origin Bloods, treatment information through Origin TRT, and internal education pages such as the TRT UK Guide and TRT Monitoring Guide.